 |
Case Series
Squamous cell carcinoma of the gallbladder
1 Department of General Surgery, AdventHealth–Orlando, Orlando, FL, USA
2 University of Miami Miller School of Medicine, Miami, FL, USA
3 Department of Pathology, AdventHealth–Orlando, Orlando, FL, USA
4 Department of Surgical Oncology, AdventHealth Cancer Institute, Orlando, FL, USA
Address correspondence to:
William Cobb
MD, General Surgery Resident, Department of General Surgery, AdventHealth–Orlando, Orlando, FL,
USA
Message to Corresponding Author
Article ID: 100107Z04WC2025
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cobb W, Caron JP, Huang R, Pernicone P, Rosales A. Squamous cell carcinoma of the gallbladder. Int J Hepatobiliary Pancreat Dis 2025;15(1):17–23.ABSTRACT
Introduction: Squamous cell carcinoma of the gallbladder (SCCGB) is an extremely rare entity, and most patients present with advanced disease at diagnosis. It has a poor prognosis with a low five-year survival rate. We present two cases with this pathology.
Case Series: Case 1: A 61-year-old female presented to our institution with five days of altered mental status, jaundice, and abdominal pain. Initial laboratory work showed evidence of biliary obstruction, severe hypercalcemia, and severe leukocytosis. Computer tomography scan (CT) and magnetic resonance cholangiopancreatography (MRCP) showed an infiltrating mass at the gallbladder neck and hepatic hilum resulting in severe intrahepatic biliary ductal dilation with metastatic adenopathy along with concern for spine and pelvis metastasis. Endoscopic ultrasound (EUS) with fine needle aspiration (FNA) was positive for invasive poorly differentiated squamous cell carcinoma. Parathyroid hormone (PTH)-related peptide was elevated. The patient expired during the hospital admission. Case 2: A 74-year-old male presented to our institution with right upper quadrant abdominal pain for one month. Liver enzymes and inflammatory markers were within normal limits. Computed tomography (CT) scan and gallbladder ultrasound (US) showed a significantly distended gallbladder with wall thickening and a focal mass like area present in the body of the gallbladder. Hepatobiliary iminodiacetic acid (HIDA) scan showed non-visualization of the gallbladder worrisome for acute cholecystitis. The patient underwent laparoscopic cholecystectomy with laparoscopic wedge liver biopsy. Pathology was significant for moderately differentiated invasive squamous cell carcinoma. The patient elected for hospice care and was lost to further follow-up.
Conclusion: Squamous cell carcinomas of the gallbladder are extremely rare tumors, and the pathogenesis is not well understood. These cancers can closely resemble gallbladder adenocarcinomas but are thought to grow quicker. Although treatment options are improving, SCCGB continues to have a very poor prognosis. More research should be done to gain a better understanding of the disease process and possible curative treatment options.
Keywords: Biliary cancer, Cholecystectomy, Gallbladder cancer, Squamous cell carcinoma
Introduction
Gallbladder cancer is the fifth most common cancer of the gastrointestinal tract and the most common primary cancer of the hepatobiliary tract, comprising 80–90% of primary hepatobiliary malignancies [1],[2]. Lee et al. reported that from 1985 to 2005, the incidence of gallbladder cancer in the United States was 0.9 per 100,000 males and 1.6 per 100,000 females, accounting for 0.16% and 0.39% of all cancers, respectively [3]. Although treatment options are improving, gallbladder cancer continues to have a poor prognosis, with an overall mean survival of six months after diagnosis, and a 5-year survival of 5% [4].
The gallbladder’s lack of submucosa contributes to the aggressive nature of the disease, with high rates of metastatic invasion [4]. Types of gallbladder cancer include adenocarcinoma, papillary carcinoma, squamous cell carcinoma (SCCGB), neuroendocrine tumors, small cell cancer, lymphoma and sarcoma with adenocarcinoma being the most prevalent histopathologic subtype [5],[6],[7]. The purpose of this case series and literature review is to provide a single institution review of documented cases of SCCGB and overview of SCCGB.
CASE SERIES
Case 1
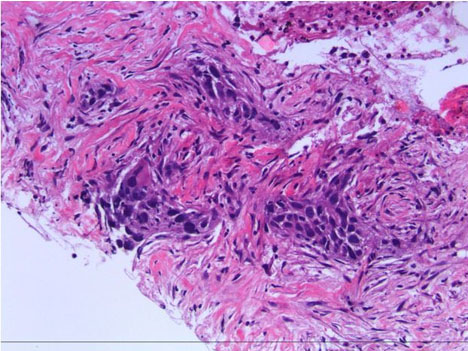
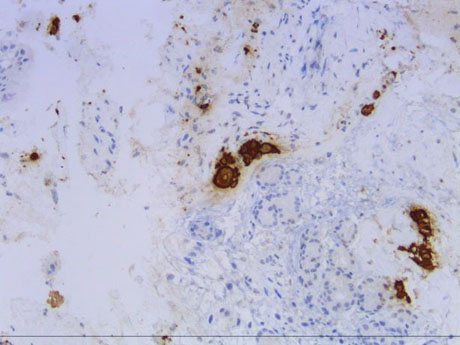
A 61-year-old female with past medical history of locally advance, triple negative adenocarcinoma of the left breast status post left-sided mastectomy and chemoradiation presented to our institution with five days of altered mental status, jaundice, and abdominal pain. Initial laboratory work showed evidence of biliary obstruction (total bilirubin of 12.4 mg/dL), severe hypercalcemia (Ca of 16.8 mg/dL), and severe leukocytosis (38.9 103/uL)). Cancer antigen 19-9 value was less than 0.6 U/mL. Parathyroid hormone (PTH)-related peptide value was 8.5 pmol/L. Computed tomography (CT) scan showed an ill-defined infiltrating mass at the gallbladder neck and hepatic hilum resulting in severe intrahepatic biliary ductal dilation (Figure 1). Subsequent magnetic resonance cholangiopancreatography (MRCP) showed 3.9 cm infiltrative mass involving the gallbladder neck, moderate intrahepatic biliary ductal dilation at the level of obstruction, and metastatic periportal, retrocrural, and retroperitoneal adenopathy (Figure 2). Both CT and MRCP were concerning for spine and pelvis metastasis. An endoscopic retrograde cholangiopancreatography (ERCP) was performed with sphincterotomy and common bile duct stent placement. Endoscopic ultrasound (EUS) with fine needle aspiration (FNA) was positive for invasive poorly differentiated squamous cell carcinoma. Immunohistochemical stains positive for CK5/6, CK7, p40, and GATA3 and negative for p16 (Figure 3 and Figure 4). Once diagnosis and staging were concluded, based on the presence of metastatic disease, the patient was evaluated by Oncology and had a port placement for systemic therapy. Repeat CT scan showed new areas suspicious for omental disease. The patient later expired within the same admission without surgical intervention.
Case 2
A 74-year-old male with history of aortic valve replacement and mitral valve replacement, atrial fibrillation, abdominal aortic aneurysm, gastroesophageal reflux disease (GERD), hypertension, and bilateral inguinal hernia repair presented to our institution with right upper quadrant abdominal pain for one month. Liver enzymes including total bilirubin were within normal limits and did not have leukocytosis. Computed tomography scan showed a significantly distended gallbladder with wall thickening and a focal mass like area present in the body of the gallbladder. Subsequently an ultrasound of the gallbladder showed findings concerning for acute cholecystitis with solid mass of 4.2 × 3.8 cm along the anterior wall of the gallbladder. Hepatobiliary iminodiacetic acid (HIDA) scan showed non-visualization of the gallbladder worrisome for acute cholecystitis. At this point, with concern for acute cholecystitis with possible gallbladder mass the patient underwent laparoscopic cholecystectomy with laparoscopic wedge liver biopsy. Pathology was significant for moderately differentiated invasive squamous cell carcinoma invading the perimuscular connective tissue with extensive lymphovascular invasion with liver wedge biopsy also positive for moderately differentiated invasive squamous cell carcinoma (Figure 4). Upon learning of pathological diagnosis the patient declined any further treatment and elected for hospice care. This patient was lost to further follow-up.



Discussion
Squamous cell carcinoma of the gallbladder background, histology, and etiology
Squamous cell carcinoma of the gallbladder (SCCGB) can be diagnosed when majority of cells within a lesion are squamous cell carcinoma with less than 10% being adenocarcinoma cells. Lesions can be referred to as squamous versus adenosquamous carcinoma based on the relative proportion of squamous cells [8]. The cutoff for proportion of squamous cells remains arbitrary. Some definitions consider adenosquamous carcinomas to be malignancies where squamous elements compromise greater than 25% of tumor specimens [9]
Squamous areas of differentiation are characterized by high expression of nuclear tumor protein p63 (TP63) and high molecular weight keratinization, while glandular tissue show high expression of monoclonal carcinoembryonic antigen (mCEA) and tumor associated glycoprotein 72 (TAG72) [10]. Mutations in k-RAS have been reported in between 39% and 59% of patients with gallbladder carcinoma although a higher frequency between 50% and 83% has been reported in patients with associated anomalous pancreatobiliary duct junction. Abnormalities of the p53 gene are seen in 35–92% of gallbladder cancer and an overexpression of p53 is associated with grade, stage, and presence of gallstones [11]. Squamous cell carcinoma of the gallbladder tumors share histological traits that are characteristic of squamous tumors at other sites, showing sheets and whorls of keratinized squamous epithelial cells with characteristic intercellular bridges and fibrous stroma [12]. Like other forms of aggressive malignancy, SCCGB can display lymphovascular invasion and perineural invasion [5]. Pure squamous cell carcinoma of the gallbladder is a type of SCCGB that lacks a glandular component and is among the rarest of gallbladder malignancies, significantly rarer than gallbladder adenocarcinoma, representing less than 3% of all gallbladder cancers [2],[13],[14]. In 2011, Roa et al. analyzed 606 cases of resected invasive gallbladder carcinoma at their institution and found that the rate of pure SCCGB was 1% [15].
The etiology of SCCGB remains poorly understood but is thought to arise from squamous cell metaplasia that results from chronic inflammation [16]. Specific theories include malignant transformation of heterotopic or metaplastic squamous epithelium or squamous metaplasia of adenocarcinoma [17]. The frequent appearance of adenocarcinoma and squamous cell carcinoma (SCC) in the same lesion supports the idea that SCC could emerge from squamous differentiation of preexisting adenocarcinoma [18]. However, the rare but explicit diagnosis of pure squamous metaplasia suggests that SCC can also arrive through de novo squamous differentiation of previously normal gallbladder epithelium [19]. Identified risk factors for SCCGB include gallstones, adenomas, porcelain gallbladder, cholecystoenteric fistula, ulcerative colitis, and anomalous biliopancreatic junction [20].
Presentation
Squamous cell carcinoma of the gallbladder displays a 3:1 female predominance and most often presents after the 5th decade of life [15]. It most frequently presents as right upper quadrant pain followed by a right hypochondrial mass and jaundice [21]. Gallbladder cancer should be suspected in a patient with gallstones with a sudden change in symptoms [11]. Jaundice is an ominous symptom at presentation that correlates highly with advanced disease, positive surgical margins, and decreased median disease-specific survival [22]. Differential diagnosis of SCCGB includes gallbladder polyp or volvulus, thickening or edema of the gallbladder (GB) wall, cholecystitis, bile duct tumors, biliary obstructions of additional nature, and other forms of gallbladder cancer [6].
Laboratory associations include anemia, hyperbilirubinemia, elevations in serum alkaline phosphatase, carcinoembryonic antigen, and/or CA 19-9 [23],[24]. Computed tomography scan or magnetic resonance imaging/magnetic resonance cholangiopancreatography (MRI/MRCP) with or without US are used for imaging workup with CT and MRI being the most sensitive and specific tests for diagnosing GB cancer [25]. Radiographic findings suspicious for gallbladder cancer include intraluminal mass, diffuse mural thickening, mass replacing the gallbladder, intra-hepatic ductal dilation, and hepatic lesions next to gallbladder fossa [26]. Ultrasound can also be used to detect features of SCCGB which include mural wall thickening or calcification, mass protruding into lumen, fixed gallbladder mass, or loss of interface between the gallbladder and liver; these findings should prompt additional studies with CT or MRI/MRCP [27]. Upper endoscopy may be superior to transabdominal US in detecting GB cancer [28]. Computed tomography scan of the chest is generally recommended to detect metastasis after initial diagnosis. Guidelines for positron emission tomography (PET) scans are unclear in the metastatic workup of SCCGB [29]. Although laboratory values and imaging evidence can contribute to diagnosis, the mainstay of SCCGB is achieved through subsequent tissue biopsy, usually performed intraoperatively [30].
Deng et al. suggest that some cancer patients present with systemic inflammatory response, which could be detected by change of peripheral blood cell amounts. Based on the count of circulating inflammatory cells, several prognostic biomarkers such as neutrophil to lymphocyte ratio (NLR) [20],[21] derived neutrophil to lymphocyte ratio (dNLR), platelet to lymphocyte ratio (PLR), and lymphocyte to monocyte ratio (LMR) have been developed to predict patient outcome in various carcinomas [24].
Treatment
Complete surgical resection offers the only chance for cure in gallbladder cancer, although surgical treatment is only an option for 10–30% of cases due to the significant portion of patients who present with unresectable disease at diagnosis [11]. Surgical options for SCCGB include simple cholecystectomy; radical or extended cholecystectomy involving removal of gallbladder plus at least 2 cm of the gallbladder bed, and dissection of lymph nodes from the hepatoduodenal ligament behind the second part of the duodenum and head of the pancreas; radical cholecystectomy with liver segment or lobar resection; radical cholecystectomy with extensive lymph-node dissection including para-aortic lymph nodes; radical cholecystectomy with resection of the bile duct or pancreaticoduodenectomy; and any of the above surgical options in addition to resection of port sites in patients who were initially treated with a laparoscopic cholecystectomy [11]. Relative contraindications to surgical resection include presence of metastases, ascites, extensive involvement of the hepatoduodenal ligament, envelopment of major vessels and poor patient performance status. Palliative procedures to relieve pain include bilioenteric bypass and endoscopic or percutaneous stenting [23]. Due to the relatively low incidence of lymphatic invasion, there is no standardized guidelines concerning lymphadenectomy in invasive SCCGB but should be considered for invasive disease. Survival rates after curative surgical resection are comparable in SCCGB and adenocarcinoma [12]. Kalayarasan et al. performed a retrospective analysis of gallbladder cancer patients who underwent gallbladder resection with curative intent between August 2009 and March 2012 and found that, compared to gallbladder adenocarcinoma, SCCGB had significantly greater tumor size and incidence of adjacent organ involvement and significantly less node positive disease and metastatic spread, despite comparable median survival after curative resection [9]. The use of adjuvant chemoradiation in combination with surgery is yet to be identified, although it has been suggested that adjuvant chemoradiation may improve disease-free survival and decrease locoregional failure [31] .
Prognosis
Like gallbladder adenocarcinoma, SCCGB shares a dismal prognosis, largely due to the late presentation of the disease; only approximately 20% of GB carcinomas present at an early stage [32]. How the two malignancies compare in terms of prognosis remains controversial. Ayabe et al. retrospectively compared outcomes of 1,084 patients with SCCGB with 23,958 patients with GB adenocarcinoma and found that SCCGB patients were diagnosed at a later stage, had higher-grade tumors at diagnosis, and had a higher margin of positivity after surgical resection, although were more likely to undergo surgery [33]. The aggressive local invasion of SCCGB is thought to be a result of its high proliferative index, low doubling time and late diagnosis when compared to gallbladder adenocarcinoma [9]. The growth rate of the squamous component of gallbladder cancer is thought to grow two times faster than the glandular component, with a doubling time of 81 days compared to 166, possibly contributing to the larger tumor size of SCCGB at diagnosis [34].
Although some argue that SCCGB represents a more ominous diagnosis than gallbladder adenocarcinoma, others argue that prognosis is comparable between the two due to SCCGB growing locally with little visceral or lymph node involvement [16]. Kalayarasan et al. retrospectively compared 122 patients with gallbladder adenocarcinoma to 14 patients with squamous cell carcinoma who underwent surgery with curative intent and found that patients in the squamous cohort presented at a higher tumor stage but had less incidence of nodal involvement and distant metastasis [9]. Pathologic stage of disease is the strongest predictor of prognosis in GB cancer in addition to factors including high tumor grade, low tumor acid mucopolysaccharide, and increased serum lactate dehydrogenase [11].
Prognostic histopathological tumor markers of SCCGB are still being elucidated and may overlap with those of adenocarcinoma of the gallbladder. Liu et al. evaluated 46 SCCGB and 80 gallbladder adenocarcinomas and found that for both types of cancer, expressions of tumor susceptibility gene (TSG) 101 and PEG20 expression were significantly associated with tumor size and TNM stage [35]. Likewise, Chen et al. analyzed 46 SCCGB and 80 gallbladder adenocarcinomas and found that expression of promothysin a (PTMA) and parathympsim (PTMS) are associated with higher tumor size and TNM stage [6]. Zou et al. analyzed tumor samples using immunohistochemistry in 46 squamous and 80 adenocarcinoma patients and found that expression of CCT2 and PDIA2, two genes encoding chaperone folding proteins, were associated with larger tumors, higher TNM staging, poor differentiation, and near tissue invasion [3],[36]. Immunohistochemistry techniques have been implemented in attempts to identify diagnostic and prognostic biomarkers of SCCGB. Li et al. investigated DDR2 and IFITM1, two genes that regulate matrix metalloproteinase expression, in SCCGB and adenocarcinoma and found that increases in these genes significantly correlated with higher TMN stages, invasion, metastasis, and prognosis across SCCGB and gall bladder adenocarcinoma [8]. As previously mentioned, gallbladder cancer continues to have a poor prognosis, with an overall mean survival of six months after diagnosis, and a 5-year survival of 5% [4].
Conclusion
Squamous cell carcinomas of the gallbladder are extremely rare tumors, and the pathogenesis is not well understood. These cancers can closely resemble gallbladder adenocarcinomas but are thought to grow quicker. Although treatment options are improving, SCCGB continues to have a very poor prognosis. More research should be done to gain a better understanding of the disease process and possible curative treatment options. Research focusing on genetics, biomarkers, and early detection methods could promote earlier identification of this disease process. Further focus on targeted and systemic therapies could improve definitive surgical resection leading to improved prognosis and patient outcomes.
REFERENCES
1.
Rakić M, Patrlj L, Kopljar M, et al. Gallbladder cancer. Hepatobiliary Surg Nutr 2014;3(5):221–6. [CrossRef]
[Pubmed]

2.
Wernberg JA, Lucarelli DD. Gallbladder cancer. Surg Clin North Am 2014;94(2):343–60. [CrossRef]
[Pubmed]
3.
Lee SW, Baek SY, Sung SH. Combined undifferentiated and neuroendocrine carcinomas of the gallbladder appearing as two separate lesions: A case report with radiological-pathological correlation. J Radiol Case Rep 2015;9(5):14–21. [CrossRef]
[Pubmed]
4.
Hundal R, Shaffer EA. Gallbladder cancer: Epidemiology and outcome. Clin Epidemiol 2014;6:99–109. [CrossRef]
[Pubmed]
5.
Takahashi H, Irri A, Fenig Y, Byale A, Thung S, Gunasekaran G. Systematic review of squamous cell carcinoma of the gallbladder. Am J Surg 2022;224(3):863–8. [CrossRef]
[Pubmed]
6.
Chen K, Xiong L, Yang Z, Huang S, Zeng R, Miao X. Prothymosin-α and parathymosin expression predicts poor prognosis in squamous and adenosquamous carcinomas of the gallbladder. Oncol Lett 2018;15(4):4485–94. [CrossRef]
[Pubmed]
7.
Ren X, Jiang H, Sun K, et al. Mixed neuroendocrine-non- neuroendocrine neoplasm of the gallbladder: Case report and literature review. Diagn Pathol 2022;17(1):51. [CrossRef]
[Pubmed]
8.
Li J, Yang ZL, Zou Q, et al. Squamous cell/adenosquamous carcinomas and adenocarcinomas of the gallbladder: An immunohistochemistry study of prognostic markers. Pathol Oncol Res 2014;20(2):285–92. [CrossRef]
[Pubmed]
9.
Kalayarasan R, Javed A, Sakhuja P, Agarwal AK. Squamous variant of gallbladder cancer: Is it different from adenocarcinoma? Am J Surg 2013;206(3):380–5. [CrossRef]
[Pubmed]
10.
Odze RD, Goldblum JR. Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas. Elsevier; 2024.
11.
Misra S, Chaturvedi A, Misra NC, Sharma ID. Carcinoma of the gallbladder. Lancet Oncol 2003;4(3):167–76. [CrossRef]
[Pubmed]
12.
Kim WS, Jang KT, Choi DW, et al. Clinicopathologic analysis of adenosquamous/squamous cell carcinoma of the gallbladder. J Surg Oncol 2011;103(3):239–42. [CrossRef]
[Pubmed]
13.
Junior MAR, de Lima Favaro M, Santin S, Silva CM, Iamarino APM. Giant squamous cell carcinoma of the gallbladder: A case report. World J Clin Cases 2019;7(18):2787–93. [CrossRef]
[Pubmed]
14.
Waisberg J, Bromberg SH, Franco MI, Yamagushi N, dos Santos PA, Castro MA. Squamous cell carcinoma of the gallbladder. Sao Paulo Med J 2001;119(1):43. [CrossRef]
[Pubmed]
15.
Roa JC, Tapia O, Cakir A, et al. Squamous cell and adenosquamous carcinomas of the gallbladder: Clinicopathological analysis of 34 cases identified in 606 carcinomas. Mod Pathol 2011;24(8):1069–78. [CrossRef]
[Pubmed]
16.
Khaira HS, Awad RW, Thompson AK. Squamous cell carcinoma of the gallbladder presenting with a biliarycolic fistula. Eur J Surg Oncol 1995;21(5):581–2. [CrossRef]
[Pubmed]
17.
Meena RN, Tiwary SK, Khanna R, Khanna AK. Primary pure squamous cell carcinoma of gallbladder: A rare entity. World J Surg Res 2015;4:18–21.
18.
Hanada M, Shimizu H, Takami M. Squamous cell carcinoma of the gallbladder associated with squamous metaplasia and adenocarcinoma in situ of the mucosal columnar epithelium. Acta Pathol Jpn 1986;36(12):1879–86. [CrossRef]
[Pubmed]
19.
Roppongi T, Takeyoshi I, Ohwada S, et al. Minute squamous cell carcinoma of the gallbladder: A case report. Jpn J Clin Oncol 2000;30(1):43–5. [CrossRef]
[Pubmed]
20.
Jena SS, Meher D. Squamous cell carcinoma of the gallbladder masquerading liver abscess with review of literature. Int J Surg Case Rep 2022;90:106710. [CrossRef]
[Pubmed]
21.
Kamat R, Pandya JS, Jashnani K, et al. Primary squamous cell carcinoma of gallbladder presenting as empyema. Bombay Hospital Journal 2001;43:447–48.
22.
Hawkins WG, DeMatteo RP, Jarnagin WR, Ben-Porat L, Blumgart LH, Fong Y. Jaundice predicts advanced disease and early mortality in patients with gallbladder cancer. Ann Surg Oncol 2004;11(3):310–5. [CrossRef]
[Pubmed]
23.
Kais H, Hershkovitz Y, Sandbank J, Halevy A. Port site metastases in squamous cell carcinoma of the gallbladder. Isr Med Assoc J 2014;16(3):177–9.
[Pubmed]
24.
Deng Y, Zhang F, Yu X, Huo CL, Sun ZG, Wang S. Prognostic value of preoperative systemic inflammatory biomarkers in patients with gallbladder cancer and the establishment of a nomogram. Cancer Manag Res 2019;11:9025–35. [CrossRef]
[Pubmed]
25.
Rooholamini SA, Tehrani NS, Razavi MK, et al. Imaging of gallbladder carcinoma. Radiographics 1994;14(2):291–306. [CrossRef]
[Pubmed]
26.
Furlan A, Ferris JV, Hosseinzadeh K, Borhani AA. Gallbladder carcinoma update: Multimodality imaging evaluation, staging, and treatment options. AJR Am J Roentgenol 2008;191(5):1440–7. [CrossRef]
[Pubmed]
27.
Pandey M, Sood BP, Shukla RC, Aryya NC, Singh S, Shukla VK. Carcinoma of the gallbladder: Role of sonography in diagnosis and staging. J Clin Ultrasound 2000;28(5):227–32. [CrossRef]
[Pubmed]
28.
American Society for Gastrointestinal Endoscopy (ASGE) Standards of Practice Committee; Anderson MA, Appalaneni V, et al. The role of endoscopy in the evaluation and treatment of patients with biliary neoplasia. Gastrointest Endosc 2013;77(2):167–74. [CrossRef]
[Pubmed]
29.
Valle JW, Borbath I, Khan SA, et al. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2016;27(Suppl 5):v28–37. [CrossRef]
[Pubmed]
30.
Willson CM, Barsoum N, Khan MTA, Rushton J. Primary squamous cell carcinoma of gallbladder with hepatic invasion. Cureus 2023;15(3):e35795. [CrossRef]
[Pubmed]
31.
Mallick S, Benson R, Julka PK, Rath GK. Adjuvant chemoradiotherapy for squamous cell carcinoma of gallbladder. J Gastrointest Cancer 2014;45 Suppl 1:237–40. [CrossRef]
[Pubmed]
32.
Blumgart LH. Tumors of the Gallbladder Surgery of the Liver, Biliary Tract, and Pancreas. 4ed. Elsevier Saunders; Philadelphia: PA, 2007. p. 764–781.
33.
Ayabe RI, Wach MM, Ruff SM, et al. Gallbladder squamous cell carcinoma: An analysis of 1084 cases from the National Cancer Database. J Surg Oncol 2020;122(4):716–722. [CrossRef]
[Pubmed]
34.
Charbit A, Malaise EP, Tubiana M. Relation between the pathological nature and the growth rate of human tumors. Eur J Cancer (1965) 1971;7(4):307–15. [CrossRef]
[Pubmed]
35.
Liu Z, Yang Z, Liu D, et al. TSG101 and PEG10 are prognostic markers in squamous cell/adenosquamous carcinomas and adenocarcinoma of the gallbladder. Oncol Lett 2014;7(4):1128–38. [CrossRef]
[Pubmed]
36.
Zou Q, Yang ZL, Yuan Y, et al. Clinicopathological features and CCT2 and PDIA2 expression in gallbladder squamous/adenosquamous carcinoma and gallbladder adenocarcinoma. World J Surg Oncol 2013;11:143. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
William Cobb - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jesse Pittard Caron - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ruiyang Huang - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Peter Pernicone - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Armando Rosales - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2025 William Cobb et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}