 |
Case Report
Surgical management of Mirizzi syndrome during the pandemic in a COVID 19 referral center: Report of a case from a developing country
1 Resident-in-Training, Department of Surgery, University of the Philippines-Philippine General Hospital, Philippines
2 Professor and Chair, Department of Surgery, University of the Philippines-Philippine General Hospital, Philippines
3 Professor, Department of Surgery, University of the Philippines-Philippine General Hospital, Philippines
Address correspondence to:
Anthony R Perez
University of the Philippines Philippine General Hospital, Taft Ave., Manila,
Philippines
Message to Corresponding Author
Article ID: 100093Z04BV2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Viray BAG, Arcilla CE, Perez AR, Venida VNA, Limpin ET. Surgical management of Mirizzi syndrome during the pandemic in a COVID 19 referral center: Report of a case from a developing country. Int J Hepatobiliary Pancreat Dis 2020;10: 100093Z04BV2020.ABSTRACT
Mirizzi syndrome (MS) is a rare complication of gallstone disease. Surgical management may be complex, depending on the type of Mirizzi, and may range from simple cholecystectomy to a hepaticojejunostomy. A 39-year-old female diagnosed previously to have gallstones was admitted in the Philippine General Hospital (PGH), a tertiary COVID 19 referral center presenting with obstructive jaundice, right upper quadrant pain and fever. Hepatobiliary ultrasonography demonstrated a markedly distended gallbladder with a stone at the Hartmann’s pouch. A diagnosis of Mirizzi syndrome with cholangitis was made. The patient was managed with broad spectrum antibiotics and scheduled for surgery. No further imaging or endoscopy was requested due to the limitations brought about by the pandemic. Upon a negative COVID 19 polymerase chain reaction (COVID 19 PCR) test result she underwent surgery, subtotal cholecystectomy, intraoperative cholangiography, and choledochoplasty. No perioperative complications were noted. This patient was managed with the goal of providing excellent patient care while limiting risks from COVID 19 both to the patient and the health care team. This case demonstrates the need to address issues brought about by the pandemic resulting in limitations in resources, added risk of morbidity to patients, and increased level of technical difficulty particularly in biliary surgery.
Keywords: COVID-19, General surgery, Hepatobiliary surgery, Mirizzi syndrome
Introduction
Mirizzi syndrome (MS) is a relatively rare benign obstruction of the common hepatic duct from an impacted gallstone in the cystic duct or infundibulum of the gallbladder causing obstructive jaundice seen in less than 1% of cholecystectomies [1],[2],[3]. Operative management of this biliary condition is a true surgical challenge even for the most technically competent, with reported post-operative surgical mortality rates of 8%. Surgical management depends on the type of Mirizzi with cholecystectomy for Type I and some Type II MS with more severe types requiring hepaticojejunostomy, particularly cases where the stone has eroded and destroyed more than two-thirds of the bike duct circumference. Patients presenting in cholangitis may benefit from preoperative drainage and control of infection prior to any definitive surgical treatment to decrease complication [1],[4]. Outcomes may be dependent not only on severity of the disease but on the endoscopist or surgeon expertise and institutional capability as well. In this time of the COVID-19 pandemic, several factors contribute to the complexity in management, including availability and safety of healthcare workers, patient safety considerations, logistics, and resource limitations [5]. This paper aims to discuss a difficult, rare, and urgent surgical case treated during the pandemic in a low resource COVID-19 referral center in a developing country.
Case Report
A 39-year-old female sought consult at the PGH Emergency Department (ED) for severe abdominal pain. She has a 5-year history of intermittent right upper quadrant abdominal pain partially relieved by antispasmodics and pain relievers. The patient had been diagnosed to have gallstones but she declined surgery due to financial constraints. Four days prior to the admission, she experienced severe right upper abdominal pain now associated with tea-colored urine, generalized jaundice (Figure 1), nausea, and vomiting but with no associated fever or acholic stools. The patient was unable to consult immediately due to the community quarantine lockdowns instituted as measures against COVID-19 community transmission.
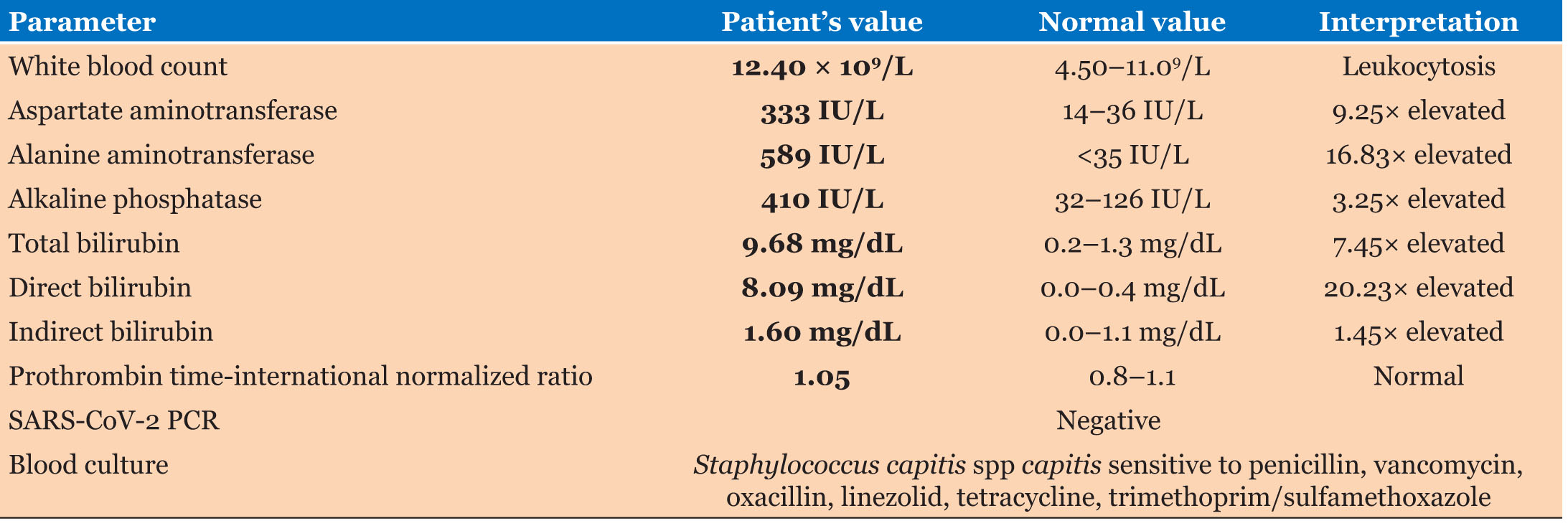
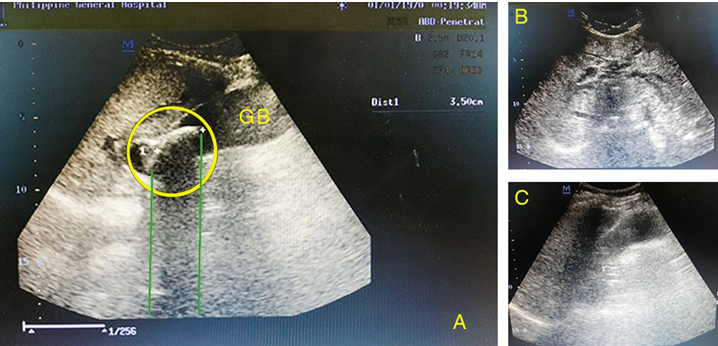
On presentation at the ED, she was alert, awake, coherent, tachycardic, normotensive, and afebrile. She had icteric sclerae (Figure 1) with right upper quadrant and epigastric tenderness. The rest of the examination was unremarkable. Initial laboratory report (Table 1) revealed leukocytosis, hyperbilirubinemia, elevated aminotransferases with normal prothrombin time, and electrolytes. Hepatitis titers were normal. The hepatobiliary ultrasonography (Figure 2) revealed a hydropic gallbladder with a 3.5 × 3 cm stone at the Hartmann’s pouch with markedly dilated intrahepatic ducts and common hepatic duct. The common bile duct (CBD) was normal at 0.6 cm. The patient was diagnosed as a case of obstructive jaundice secondary to MS with moderate cholangitis based on the Tokyo Guidelines 2018.
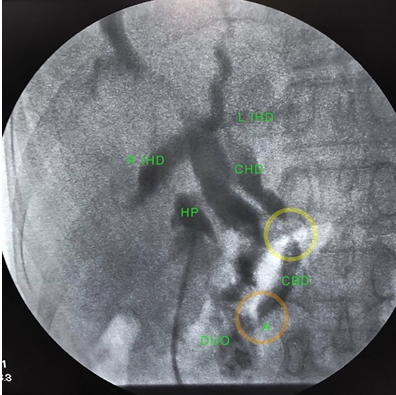
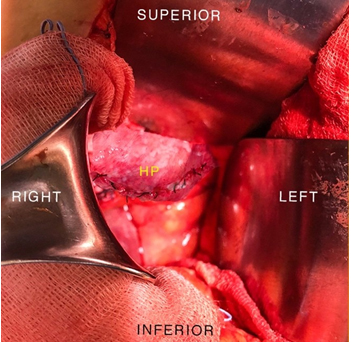
The patient was started on ceftriaxone and metronidazole along with intravenous antispasmodic and analgesics. The patient was admitted to an indeterminate ward in relative isolation while awaiting swab results. The patient was scheduled for open cholecystectomy, intraoperative cholangiography with possible CBD exploration. A COVID-19 PCR test was performed and came out negative for COVID-19 after seven days. The patient during the interim remained afebrile with normal vital signs and tolerable abdominal pain. The leukocytosis reverted to normal after four days of antibiotics. The patient underwent surgery at the non-COVID operating room. Anesthesia was administered using combined epidural and general anesthesia. Intubation was performed in an aerosol box as a precaution against aerosol production. The surgical team comprised of a senior biliary surgeon assisted by two senior residents. All were in level 4 personal protective equipment (PPE) as per recommendation for pandemic surgery during that time. A Kocher incision was used and revealed a markedly distended gallbladder with thickened walls, with dense adhesions noted in the Hartmann’s pouch and hepatoduodenal area. Careful dissection was unable to clearly identify the triangle of Calot. The team proceeded with gallbladder decompression evacuating white bile. The gallbladder was opened longitudinally for intraluminal extraction of a 3.5 × 3 cm pigment stone impacted in the Hartmann’s pouch, exposing the bile duct with yellow bile coming out (Figure 3). A French 16 Foley catheter was used to introduce contrast material with the balloon inflated in the Hartmann’s pouch and cholecystocholangiography was performed using fluoroscopy (C-arm). The intraoperative cholangiography revealed the following: dilated proximal hepatic duct, significant narrowing at the mid common bile duct, normal distal bile duct, tapering at the ampulla, and egress of dye into the duodenum (Figure 4). The team proceeded with cholecystectomy. Leaving a part of the Hartmann’s pouch intact on the lateral CBD wall. The remaining gallbladder wall was used as a flap to cover the exposed common bile duct, completing a choledochoplasty (Figure 5). The total operating time was 2.5 hours with blood loss of 200 cc. The postoperative diagnosis was obstructive jaundice from Mirizzi syndrome Type II. The final specimen is shown in Figure 6. There were no noted perioperative complications and the patient was discharged two days after surgery. Follow-up was done with the surgical team through teleconsultation. Sutures were removed after 10 days in a local health center by a general practitioner. All symptoms referable to the gallbladder disease resolved on latest follow-up two months after the surgery.



Discussion
Mirizzi syndrome (MS), though an uncommon complication of gallbladder disease, has been widely reported in the literature sine cholecystectomy is one of the most commonly performed general surgery cases. This patient presented with signs and symptoms usually associated with MS, including a classic ultrasound finding of the biliary tree. This case is being presented not only for the complexity of the surgical management but for the marked deviation from the conventional management due to the adjustment the surgical team had to make in response to the pandemic. This case was managed in a low resource tertiary COVID referral center during a time of uncertainty brought about by the pandemic, when community transmission is on the rise, hospital policies are still being formulated, engineering infection controls are yet to be in place, and standard protocols for pandemic surgery are still evolving. This experience will hopefully provide lessons to similarly situated health care centers and to other centers attending to difficult biliary cases.
Consistent with literature review, the patient presented with obstructive jaundice (60–100%) accompanied with abdominal pain over the right upper quadrant (50–100%). The most common laboratory findings with MS patients are hyperbilirubinemia, elevated aminotransferase levels, and leukocytosis which are also seen in patients with cholangitis and cholecystitis [6]. The only adjunct imaging done for the patient was ultrasound which has a diagnostic accuracy of 29% [7] with sensitivity of 8.3–27% [8],[9]. The ultrasound image we obtained for our patient, with a demonstration of a stone in the neck, dilated common and intrahepatic ducts, and a normal sized CBD are diagnostic of MS. A magnetic resonance cholangiopancreatography (MRCP) or an endoscopic retrograde cholangiopancreatography (ERCP) would have been ideal to obtain a preoperative roadmap to better prepare the surgical team and simplify intraoperative decision making. Magnetic resonance cholangiopancreatography was not available during that time and endoscopy for this case was deemed not a priority by the endoscopists due to concerns for safety and allocation of limited instrumentation. Performance of a preoperative cholangiography may have obviated the need for intraoperative fluoroscopic imaging which consequently prolonged the surgery and added to the physical stress of the patient and the entire surgical team. It likewise consumed precious operating room time shared by all the surgical specialties during this crisis situation.
The Tokyo Guidelines 2018 recommend that patients diagnosed with moderate cholangitis may have early endoscopic or percutaneous transhepatic biliary drainage [10]. Moreover, in a study done by Clemente et al., excellent outcomes are obtained with placement of one or more stents by ERCP, followed by elective cholecystectomy leaving a small portion of the gallbladder adherent to the CBD. The stent may be left in place and removed after 2 months [11]. There are those reporting good results through biliary drainage by endoscopic papillotomy and placement of biliary endoscopic stents [4]. Thus, one other option would have been to leave the stent in place and proceed with definitive management once conditions were more favorable. During this stage of the pandemic, hospital policies did not prioritize endoscopy for concerns of patient and health care worker safety. Most studies at this time have classified ERCP as an aerosol generating procedure and thus are deemed high risk procedures, regardless of COVID-19 testing results. Endoscopic procedures were allowed only for a limited subset of emergency cases like caustic ingestion and in biliary patients, severe cholangitis as advised by Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) [12].
Definitive plan for this patient was surgical intervention given the diagnosis. Options ranged from surgical biliary drainage (in the absence of percutaneous and endoscopic options) via a tube cholecystostomy or tube choledochostomy or a definitive surgical procedure. Definitive procedure may entail a cholecystectomy, common bile duct exploration, or a hepaticojejunostomy. The patient was treated with broad spectrum antibiotics, analgesics, and anti-spasmodics. The patient responded favorably with the leukocytosis resolving—white blood cell (WBC) 12.40 decreased to 7.40 and marked reduction in right upper quadrant abdominal pain. This allowed time for the team to await the results of the PCR test which came out on the 7th day. The PCR testing capability of PGH despite being the main COVID referral hospital in the country was limited at that time and the sheer volume of samples precluded immediate results. Resolution of the cholangitis with conservative management allowed the surgical team to prepare for definitive surgery. In ordinary times, waiting for a few more weeks would have allowed further reduction in the severity of inflammation. This will, however, further prolong her hospital stay and render the hospital bed unavailable to other patients. Sending her home risked losing her again to follow up and developing complications at home.
The surgical team consisted of a senior hepatobiliary surgeon and two senior residents-in-training to facilitate better intraoperative surgical dissection and decision-making. This is in contrast to pre-COVID practice of allowing junior surgical residents to perform procedures for training. In this particular case, it was anticipated that cholecystectomy for MS may pose technical challenges to the inexperienced. As recommended by experts sharing their results, the acute and chronic presentation of MS type I could be adequately resolved with cholecystectomy. More often than not, however, the dense adhesions and extensive chronic inflammation leads to distortion of Calot’s triangle and will not allow complete dissection of the Hartmann’s pouch. In our patient where the erosion involved less than a third of the circumference, reconstruction of the bile duct wall using the remnant gallbladder was possible with a choledochoplasty. In reported cases where the bile duct wall has been damaged more extensively, a hepaticojejunostomy may be required [1],[3],[8],[11]. The team elected not to put a T-tube in place since the tissues were deemed not markedly inflamed. This will likewise reduce hospital visits and relieve the patient of tube care during the time of the pandemic.
Surgery is the definitive management for MS but may pose challenges even for experienced biliary surgeons for several reasons. First, there is a low index of suspicion for this condition among surgeons since MS is not commonly seen since gallstone diseases are usually managed before MS sets in. Second, preoperative diagnosis is often not established, thus rendering the team unprepared. Third, distortion of the anatomy by dense adhesions due to longstanding inflammation and the presence of the chole enteric fistula increases the risk of bile duct injury or massive hemorrhage during dissection of the Calot triangle. Furthermore, inflammation can cause cutaneous fistula, secondary biliary cirrhosis, delayed onset biliary strictures, and even death.
An open surgical approach was chosen due to its relative safety when compared with the laparoscopic technique which is associated with high conversion rates (31–100%) and an increased incidence of bile duct injury. The open laparotomy approach has the advantage of better visualization, haptic feedback, and gallbladder calculus removal before cholecystectomy despite its more invasive nature, high complication rate, and longer postoperative hospital stay. In the era of the pandemic, laparoscopy was initially discouraged due to the aerosol generating nature of the procedure. Recently, the emergence of equipment like smoke evacuators and similar pneumoperitoneum filtering devices have increased the utilization of laparoscopy.
The practice of surgery is on standstill during this time of COVID crisis internationally. Surgeries have been limited to emergencies, mainly for life and limb threatening procedures. This has been more pronounced in countries where community transmission has exerted tremendous pressure on health care systems. In the Philippines where the most number of cases in Southeast Asia are being reported, tertiary government facilities such as the Philippine General Hospital (PGH) have been designated as COVID referral centers to address the expected influx of critically affected patients. Despite the difficulty, the PGH struggled to maintain its capability to serve surgical patients requiring treatment. New protocols in surgical practice were formulated to handle surgical cases during the time of COVID and when it is restarted after the crisis [13]. The American College of Surgeons (ACS) [14] and SAGES [12] have issued guidelines and COVID-19 precautions in the operating room. Such guidelines are important, but degree of compliance will be highly dependent on local conditions, availability of resources, and institutional limitations. One such guideline was issued by the Philippine Association for Hepato-Pancreato-Biliary Surgeons (PAHPBS), stating that cases such as biliary obstruction that may cause sepsis is highest priority should be given priority during this time of crisis due to the imminent rise of early mortality [15]. The group of Strasberg and Hughes likewise emphasizes the prioritization of emergency and urgent life-threatening cases such as sepsis, cholangitis, and obstructive jaundice whether COVID or non-COVID [16]. They also published brief outline of management of symptomatic gallbladder diseases and acute cholecystitis during this pandemic. The best surgical care for patients with gallbladder disease should be provided even during the pandemic. Exposure to the coronavirus must be limited both for patients and the health care professionals caring for them. The principles were carefully followed for this case. Resources must be allocated keeping in mind the raging pandemic. Preserve resources to care for corona virus patients.
As detailed above, despite lack of access to diagnostics and therapeutic endoscopy the patient successfully underwent definitive surgery. The surgical team was composed of the most experienced residents along with the attending surgeon to expedite the operation and limit unnecessary exposure to both the patient and the surgical team. This was in preparation for the anticipated technical difficult attendant to MS and the need for accurate intraoperative decision. The radiology department likewise made sure that a technician well versed in the use of the C-arm fluoroscopy was there to assist, instead of the team relying on static cholangiography. In regular days, intraoperative cholangiography for biliary surgeries in PGH were done with static portable X-rays requiring development of films in a separate facility due to resource limitations. This is reflected on the average operating time of cholecystectomy with intraoperative cholangiography in PGH which is approximately 3 hours 40 minutes [17]. A portable fluoroscopy (Figure 4) intraoperative cholangiography was utilized to have a real time assessment of the biliary tree. It provided faster, and more efficient visualization of the surgical field, thus promoting a safer surgery to prevent bile duct injuries [18],[19],[20].
Adherence to guidelines on the use of PPE was emphasized for protection of both patients and health care workers. Among the unique challenges of doing surgery during the time of COVID are limitations to vision and tactile sensation brought about by makeshift goggles and face shields, as well as triple-layered gloves recommended by the hospital’s infection control unit during the early part of the pandemic. To minimize limitation to vision, antifog products were used on the goggles and face shields. Micropore tape was used to prevent any warm air escaping through the N-95 mask. The hospital had not acquired powered air-purifying respirator during the time of surgery.
The patient was seen via teleconsultation on follow-up. Teleconsultation is a strategy for patient encounters recommended during this time of crisis [17]. The drain was removed prior to discharge. Sutures were requested to be removed by a general practitioner in a nearby hospital to obviate the need for the patient to travel in light of the lockdown restrictions prevailing at that time. No perioperative complications were noted, and the patient was completely symptom free one month after the surgery.
The PGH repurposed its logistics to provide care to COVID patients as a COVID referral center and also service to non-COVID patients. Cohorting of patients was done to segregate patients deemed at low risk for COVID, particularly those requiring surgical intervention. The patient was admitted in a non-COVID ward abiding with World Health Organization (WHO) precautions, including engineering controls, protective equipment for patients and health care workers, and physical spacing. She was operated in a non-COVID operating room setup.
Conclusion
Mirizzi syndrome is a rare complication of gallstone disease. The management requires a careful planning and sound intraoperative decision-making. In this era of the pandemic, the challenge is not only in the complexity of the disease but in limitation of resources and the added risk of COVID to both patients and the health care team. Difficult biliary operations during times of crisis call for surgical expertise, team efficiency, logistics resourcefulness, and resiliency to have a safe surgery. An experienced surgical team with particular expertise on biliary surgery and optimization of meager resources may mitigate these challenges. The lessons learned from the management of this case may prepare us in facing similar cases in the future. Other institutions sharing their experiences in this era of the pandemic may shape the practice of surgery in similarly resource challenged institutions.
REFERENCES
1.
Hazzan D, Golijanin D, Reissman P, Adler SN , Shiloni E. Combined endoscopic and surgical management of Mirizzi syndrome. Surg Endosc 1999;13(6):618–20. [CrossRef]
[Pubmed]

2.
Leopardi LN, Maddern GJ. Pablo Luis Mirizzi: The man behind the syndrome. ANZ J Surg 2007;77(12):1062–4. [CrossRef]
[Pubmed]
3.
Haritopoulos KN, Labruzzo C, El Tayar AR, Karani J, Hakim NS. Mirizzi syndrome: A case report and review of the literature. Int Surg 2002;87(2):65–8.
[Pubmed]
4.
Uppara M, Rasheed A. Systematic review of Mirizzi’s syndrome’s management. JPO. J Pancreas (Online) 2017;18(1):1–8.
5.
Coccolini F, Perrone G, Chiarugi M, et al. Surgery in COVID-19 patients: Operational directives. World J Emerg Surg 2020;15(1):25. [CrossRef]
[Pubmed]
6.
Beltrán MA. Mirizzi syndrome: History, current knowledge and proposal of a simplified classification. World J Gastroenterol 2012;18(34):4639–50. [CrossRef]
[Pubmed]
7.
Safioleas M, Stamatakos M, Safioleas P, Smyrnis A, Revenas C, Safioleas C. Mirizzi syndrome: An unexpected problem of cholelithiasis. Our experience with 27 cases. Int Semin Surg Oncol 2008;5:12. [CrossRef]
[Pubmed]
8.
Al-Akeely MHA, Alam MK, Bismar HA, Khalid K, Al-Teimi I, Al-Dossary NF. Mirizzi syndrome: Ten years experience from a teaching hospital in Riyadh. World J Surg 2005;29(12):1687–92. [CrossRef]
[Pubmed]
9.
Yonetci N, Kutluana U, Yilmaz M, Sungurtekin U, Tekin K. The incidence of Mirizzi syndrome in patients undergoing endoscopic retrograde cholangiopancreatography. Hepatobiliary Pancreat Dis Int 2008;7(5):520–4.
[Pubmed]
10.
Miura F, Okamoto K, Takada T, et al. Tokyo Guidelines 2018: Initial management of acute biliary infection and flowchart for acute cholangitis. J Hepatobiliary Pancreat Sci 2018;25(1):31–40. [CrossRef]
[Pubmed]
11.
Clemente G, Tringali A, De Rose AM, et al. Mirizzi syndrome: Diagnosis and management of a challenging biliary disease. Can J Gastroenterol Hepatol 2018;2018:6962090. [CrossRef]
[Pubmed]
12.
Pryor A. SAGES and EAES recommendations regarding surgical response to Covid-19 crisis. 2020. [Available at: https://www.sages.org/recommendations-surgical-response-covid-19/]
13.
Liu Z, Zhang Y, Wang X, et al. Recommendations for surgery during the novel coronavirus (COVID-19) epidemic. Indian J Surg 2020;1–5. [CrossRef]
[Pubmed]
14.
American College of Surgeons. COVID-19 and surgical procedures: A guide for patients. [Available at: https://www.facs.org/covid-19/clinical-guidance/patient-guide]
15.
Teh C. The 9Ps of PAHPBS Post ECQ preparedness in COVID-19 pandemic. 2020. Available at: https://pcs.org.ph/assets/images/archives/PAHPBS-9Ps-for-ECQ_Preparedness.pdf]
16.
Strasberg S, Hughes T. BRIEF outline of management of symptomatic gallbladder disease and acute cholecystitis during the COVID-19 pan epidemic. 2020. [Available at: https://www.facs.org/-/media/files/covid19/symptomatic_gallbladder_recommendations.ashx]
17.
Hallander JE, Carr BG. Virtually perfect? Telemedicine for Covid-19. N Engl J Med 2020;382(18):1679–81. [CrossRef]
[Pubmed]
18.
World Health Organization. Addressing ethical issues in pandemic influenza planning. 2008;1–28. [Available at: https://www.who.int/csr/resources/publications/cds_flu_ethics_5web.pdf]
19.
Philippine College of Surgeons. Recommendations for the rational and effective use of personal protective equipment (PPE): guidelines for extended use, re-use and acceptable reprocessing methods. Manila: Philippine College of Surgeons; 2020. [Available at: https://pcs.org.ph/assets/images/archives/PCS-COVID-10-Rationale-Use-of-PPE.pdf]
20.
Handy JE, Rose SC, Nieves AS, Johnson RL, Hunter JG, Miller FJ. Intraoperative cholangiography: Use of portable fluoroscopy and transmitted images. Radiology 1991;181(1):205–7. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Brent Andrew G Viray - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Crisostomo E Arcilla - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Anthony R Perez - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Vincent Nestor A Venida - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Emmanuel T Limpin - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Brent Andrew G Viray et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}